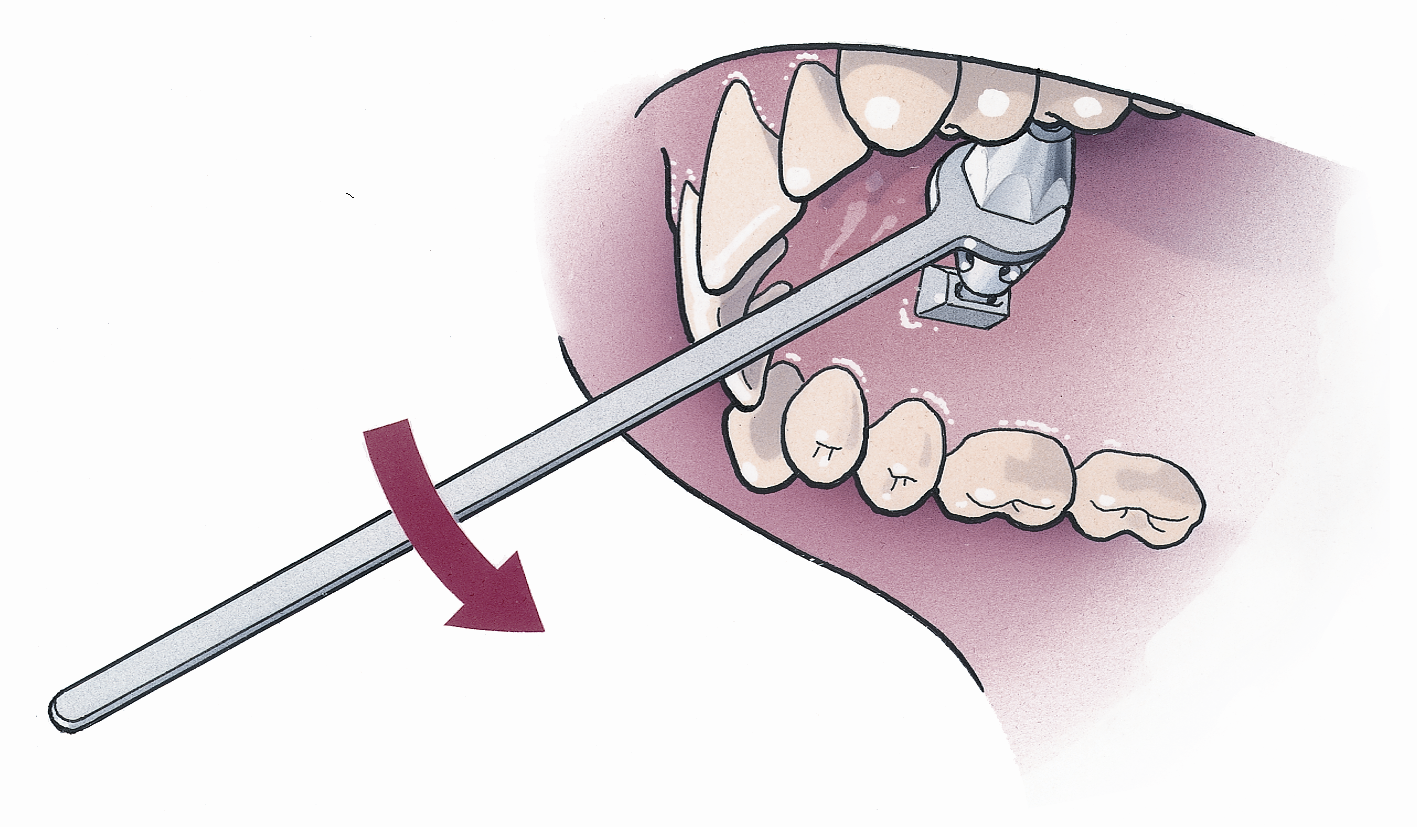
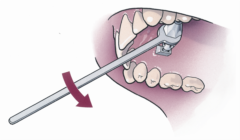
Correction of weak chin (chin advancement osteotomy)


A small chin may lead to premature aging because of a lack of support in the soft tissues in the lower face and the neck. This variance leads to the appearance of puffy cheeks, early drooping of the facial tissue in the cheek, and an abnormally large chin-neck contour angle.
Having an osteotomy (surgical procedure to shorten, lengthen or change structure of a bone) offers a predictable and permanent result, but requires receipt of general anaesthesia and a one night stay in the hospital.
Complications resulting from this procedure are rare, but 10% of the time there is a passing disruption of feeling in the lips.
The difficulty with chin advancements lies in the outline of the jaw line, which is sometimes hampered by the location of the exit of the sensory nerve.
An elastic dressing, applied after completion of the procedure, is required for one or two days. The incision is made in the mouth and is closed using sutures that break-down over time and do not require removal.
Aftercare
Cold packs are provided in the hospital and may be continued for the next 2 days at home. In addition, oral hygiene (regular brushing of teeth, flossing, etc.) is not discontinued after the procedure.
Manual lymph drainage therapy acc to Vodder is helpful in reducing swelling resulting from the collection of fluid in these areas after the procedures is completed. It is best when initiated before surgery and performed by a competent physiotherapist.
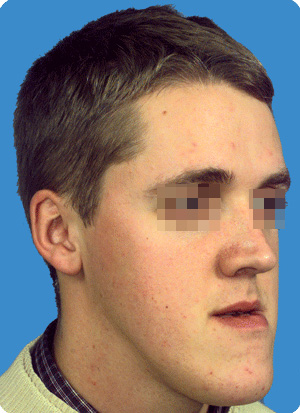
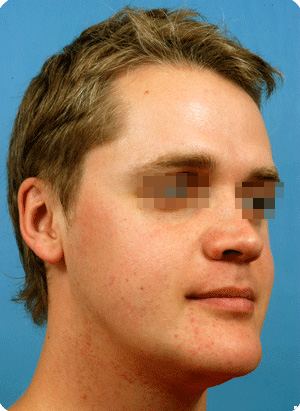
Correction of excessive show of the upper teeth due to an underdevelopment of the lower jaw (procedure performed: mandibular lengthening osteotomy)


The appearance of a face with imperfection of the lower jaw is best appreciated in the profile view. The chin is poorly defined, the front teeth are often pushed forward and the lower lip curls outward, under the forwardly projecting upper front teeth. The labio-mental indentation can be so deep, it may cause eczema (a non-contagious inflammation of the skin).
Additionally, there is a loss of support for the overlying soft tissues of the cheeks, which appear fuller than they are. The neck-chin angle is larger than normal, with a double chin appearance and early drooping of the facial tissue of the cheeks.
The facial appearance worsens with the normal aging process, due to the soft tissues lack of proper support.
The persons affected by this underdevelopment also usually have problems properly chewing solid food.
The combination of orthodontic treatment and jaw surgery (of the lower jaw and sometimes the chin) will correct both chewing comfort and facial harmony.
Lower jaw lengthening is usually done while under general anaesthesia, with a one night hospital stay. Lengthening by osteodistraction, using either local anaesthesia or in a one-day surgical clinic, are other options. Endoscopically (use of an instrument to examine the interior of the jaw visually) controlled lower jaw lengthening is pioneered.
A standard procedure causes swelling in the area of the jaw angles, lasting about 2 to 3 weeks. In addition, altered sensation or feeling in the lips can occur in 30% of the cases and is temporary, although it may last several months.
Intermaxillary fixation (dental wiring) is not required, but the patients are provided with training elastics to use between the orthodontic braces for many weeks. The incision is made in the mouth and is closed using sutures that break-down over time and do not require removal..
Two complications may occur with this procedure. Wound infection in seen less than 3% of the patients and joint pain can occur in adults, with the pain lasting up to several weeks. Rarely (less than 1 in 1000 patients), severe joint pain may warrant infiltrations.
Aftercare
Cold packs are provided in the hospital and may be continued the next 2 days at home. In addition, oral hygiene (regular brushing of teeth, flossing, etc.) is not discontinued after the procedure.
A soft diet is required for 4 to 5 weeks. This will involve the use of a blender in the first week and eating pastas for another 3 weeks.
Manual lymphe drainage therapy acc to Vodder is helpful in reducing swelling resulting from the collection of fluid in these areas after the procedures is complete. It is best when initiated before surgery and performed by a competent physiotherapist.
Correction of Long Face with Excessive Growth of the Lower Jaw (procedure performed: surgical repositioning of the upper jaw, lower jaw and chin – “trimax”)


Mandibular (lower jaw) excess is rarely corrected by a shortening of the lower jaw only. Advancement of the upper jaw, or of the chin, is required in the majority of the cases in order to avoid premature aging signs in the mid-face and the neck. Upper jaw impaction may be required to address the following: inability to close the lips without forceful action of the chin muscles, a gingival smile (more than 4 mm of gum show upon smiling) and facial disharmony (long face).
The orthodontist's goal will be to correct the poor positioning of the teeth. The surgeon's objective is to reposition the jaws to achieve a working occlusion (lining up of the upper and lower jaw) and to enhance the visual perception of the face, chewing ability, speech formation, nasal air flow, and lip closure.
Surgery in the upper jaw, lower jaw, and the chin, requires a hospital stay of two days. During the first night after the procedure, the patient is in the Midcare department for comfort reasons.
A standard “trimax” procedure causes swelling of the mid-face, the angles of the jaw and the chin area, which will last about three weeks. A change in the feeling in the lips happens in 40% of the cases and is temporary, although it may last for several months.
Intermaxillary fixation (dental wiring) is not required, but patients are provided with training elastics to use between the orthodontic braces for many weeks. The incision is made in the mouth and is closed using sutures that break-down over time and do not require removal..
Two complications may occur with this procedure. Wound infection in seen less than 3% of the patients and joint pain can occur in adults, with the pain lasting up to several weeks. Rarely (less than 1 in 1000 patients), severe joint pain may warrant infiltrations.
Aftercare
Cold packs are provided in the hospital and may be continued for the next 2 days at home. In addition, oral hygiene (regular brushing of teeth, flossing, etc.) is not discontinued after the procedure.
A soft diet is required for 4 to 5 weeks. This will involve the use of a blender in the first week and eating pastas for another 3 weeks.
Manual lymph drainage therapy acc to Vodder is helpful in reducing swelling resulting from the collection of fluid in these areas after the procedures is complete. It is best when initiated before surgery and performed by a competent physiotherapist.
Correction of Lip Incompetence (the impaction of the upper jaw and of the chin, frequently combined with forward repositioning of the lower jaw)




Long faces show a facial disharmony, inability to close the lips while the muscles are relaxed, a “mentalis habit” (excessive use of the chin muscle to bring up the lower lip), a “gingival smile” (more than 4 mm of gum show upon smiling), and evidence of a dysfunctional chewing motion.
Typically, long faces are corrected with a “trimax” procedure: upper jaw impaction, lower jaw advancement (for reasons relating to bite) and chin height reduction. All of the surgery is performed by the oral route (no skin incisions), and extra procedures may be combined.
Patients stay a minimal two days in the hospital, with the first night after surgery being spent in Midcare department.
The incision is made in the mouth and is closed using sutures that break-down over time and do not require removal. Swelling in the face may last for three weeks, after which about 10% of patients may take up to several more weeks to resolve. Changes in the feeling of the lips or cheek may occur in 30% of the patients.
Intermaxillary fixation (dental wiring) is not required, but patients are provided with training elastics to use between the orthodontic braces for several weeks.
Two complications may occur from this procedure. Wound infection in seen less than 3% of the patients and joint pain can occur in adults, with the pain lasting up to several weeks. Rarely (less than 1 in 1000 patients), severe joint pain may warrant infiltrations.
Aftercare
Cold packs are provided in the hospital and may be continued for the next 2 days at home. In addition, oral hygiene (regular brushing of teeth, flossing, etc.) is not discontinued after the procedure.
A soft diet is required for 4 to 5 weeks. This will involve the use of a blender in the first week and eating pastas for another 3 weeks.
Manual lymph drainage therapy acc to Vodder is helpful in reducing swelling resulting from the collection of fluid in these areas after the procedures is complete. It is best when initiated before surgery and performed by a competent physiotherapist.
Correction of box-shaped mandible (reduction of masseter hyperplasia)


Mandibular angles which are too prominent can be because of the muscle, the bone or both. Botox infiltrations may be of help in reducing the bulk of the muscle. A bony prominence or a combination of muscle and bony hyperplasia is addressed by performing a surgical reduction with an approach by the mouth. Typically, a lot of soft tissue swelling will be present after the procedure is completed.
Aftercare of a surgical correction
Cold packs are provided in the hospital and may be continued for the next 2 days at home. In addition, oral hygiene (regular brushing of teeth, flossing, etc.) is not discontinued after the procedure.
Manual lymph drainage therapy acc to Vodder is helpful in reducing swelling resulting from the collection of fluid in these areas after the procedures is complete. It is best when initiated before surgery and performed by a competent physiotherapist.
Mouth opening exercises will be also be prescribed.
Correction of narrow faces

Malar projection osteotomies and moldable mandibular angle augmentation create proper definition in the lateral face.
Rhinoplasty (nose job)








The nose has to fit the face. To new proportion the nose to fit the face is the responsibility of the surgeon. However, details such as whether the nose is straight or curved, has a narrow or wide dorsum or a wide or pointy nasal tip, is a matter of personal taste. Pictures in magazine are helpful when discussing these details and difficult decisions may be supported by simulation in profile view of the patient.
I hardly ever use an incision in the columella (column supporting the nasal tip). Open structure rhinoplasty is sometimes required in broad, bifid, asymmetrical or too projected nasal tips. But this can be done by a delivery technique, without the need for external incision.
After care
Internal splints (a spongy material with airway tubes) are removed after four days or after 12 days (if silicone septal splints are used). The external nasal splint (plastic nasal cap, with no plaster) is replaced after five days and is removed after 12 days.
Prolonged swelling above the nasal tip (“supratip deformity/abnormality”) may occur as the most common complication. It is often due to an excess of subcutaneous (under the skin) scarring in patients with a thick dermis (skin layer) and wide pores. To prevent this, elastic taping is required at night, and when possible also during the daytime, for at least three weeks. Supratip deformity tends not to appear when the nose starts to soften again.
Many patients like to also wear the nasal cap at night for two more weeks, as a kind of “psychological” helmet.
For further information about rhinoplasties, click here.
Lip job (lip augmentation/enhancement, smoothing of peri-oral wrinkles)


Although theoretically the safest way, augmentation with patient’s own processed fat is also quite unpredictable. Fillers made of cross-linked hyaluronic acid, a ground substance in the skin, are lasting for nearly one year.
Although most permanent fillers are relatively safe, they have a negative history with the public, due to a few dramatic cases published in the news.
Fillers may be used to increase lip volume, to decrease the wrinkles around the mouth, or for both reasons.
Dental block anaesthesia lessens the pain sensation, and for after care, petrolatum (Vaseline) is used.
It is very important to mention if you have cold sores (Herpes labialis) or the intake of blood-thinning medicines, prior to receiving these procedures.
Ear job (otoplasty or correction of bat ears)
There is wide variation in the shape of the ears. Ears that stick out or are abnormal in size make children targets for teasing. Otoplasty may be carried out as early as five years of age (with the use of general anaesthesia) or at any time during adulthood (using either local or general anaesthesia).
A hidden incision is made behind each ear, providing access to the cartilage. The cartilage is then reshaped to create an improved curvature and position.


15 years after the surgery
 15 years after the surgery
15 years after the surgery
After care
Sutures that break-down over time and do not require removal are used, and a bandage is only required at night. After this brief recovery period, the return to school or work is quick.
Enhancing smile aesthetics by gradual surgical expansion of jaws (transpalatal/transmandibular distraction osteogenesis)

Transpalatal Distraction is a technique by which the upper jaw is surgically expanded after weakening the bony pillars with key-hole surgery in the nose, and applying a transverse force on the palate on a daily base by the patient by means of a titanium distraction device fixed in the palatal vault.
Transmandibular Distraction is using a similar technique to widen the front part of the lower jaw.
Expanding the jaws result in space for the crowed front teeth, a reduction of the unattractive dark buccal corridors, and the correction of any issue with chewing, caused by cross-bite.
The devices are generally removed using local anaesthesia only.
Often, surgical expansion is a preliminary step to align the dental arches before facial reconstruction (performed either vertically or horizontally on the face).
After care
The thorough use of an antiseptic jelly, and the continuation of oral hygiene, is necessary for healthy gum conditions around the titanium abutments on the roof of the mouth.
Blowing of the nose is forbidden for three weeks, and the use of a salt water spray helps to prevent nasal obstruction.
Orthodontic Bone Anchors
These small devices allow to close unilateral diastemas, to avoid posterior movement of the front teeth and to avoid headgear appliances when orthodontic preparation for orthognathic surgery requires meticulous detailed occlusal preparation.
Click here for a slide presentation
Total facial makeover surgery
A single stage reshaping of the face, without skin incisions, addresses the following: the shape of the nose, the malar (cheek) bones, the chin, the jaw angles, the dental occlusion (lining up of the upper and lower jaw), the position of the lips, the draping of the soft tissues in the neck and the mandibular border (jaw line), and the emphasis of shadow lines and highlights. As such, it is possible to transform an ugly duck into a swan.
Facial makeover surgery is made known to the public through certain television programs. The commercial approach; however, does not always equal the evidence based approach. The latter tries to avoid the use of prosthetic (manufactured) materials to address irregularities, such as facial implants or dental bridges, whenever possible. Orthodontic treatment and two-phase surgery may be needed to provide a long-lasting and optimal result.
Facial makeover surgery, or facial transformation surgery, combines the above mentioned osteotomy and soft tissue procedures with bony strengthening surgery, and complementary fat grafting.
















After care
Swelling is considerable after the procedure and will keep the patient from social interactions for at least two weeks. Facial makeover provides a major boost of self confidence; however, the change may be so dramatic that patients have problems recognising themselves in the mirror for a couple of months. Psychological counselling is highly recommended before the surgery, because emotional support may be required after the surgery.
Annex I - Orthognathic Surgery Brochure.pdf
| Back |